
- BACKGROUND
The landmark introduction of The Misuse of Drugs (Amendments) (Cannabis and Licence Fees) (England, Wales and Scotland) Regulations 2018 [1]paved the way for legalised access to medicinal cannabis in the UK. Medicinal cannabis was subsequently defined as a special medicinal product which could be used in accordance with a prescription.
Products are classed as cannabis-based products for medicinal use (CBPMs) under Regulation 2(1) of the Misuse of Drugs Regulations 2001[2] (as amended), if they satisfy the following three requirements:
- The product is or contains cannabis, cannabis resin, cannabinol or a cannabinol derivative
- It is produced for medicinal use in humans; and
- It is a product that is regulated as a medicinal product, or an ingredient of a medicinal product.
- WHO CAN PRESCRIBE
The initial prescription of a CBPM must be made by a doctor included on the register of specialist practitioners. It is also expected that the practitioner will have a special interest in the condition being treated, within their own practice and training, for example, in the case of treatment of drug-resistant epilepsy in children, any prescribing would be expected to be initiated by tertiary paediatric neurologists as advised by NICE in their guidance[3].
Licensed CBPM’s
To date, within the UK, there are only two CBPMs, Sativex (nabiximols) and Epidyolex (highly purified cannabidiol, ‘CBD’) and one synthetic cannabinoid, Nabilone, which have received a UK marketing authorisation (product licence)[4].
In the NHS, funding for these medicines is a decision for local integrated care boards[5], this can create a ‘post-code lottery’ for those looking to benefit from the licensed CBPM’s.
Unlicensed CBPMs
The Medicines & Healthcare products Regulatory Agency (MHRA) has issued guidance regarding the import and use of unlicensed or ‘specials’ CBMP’s[6].
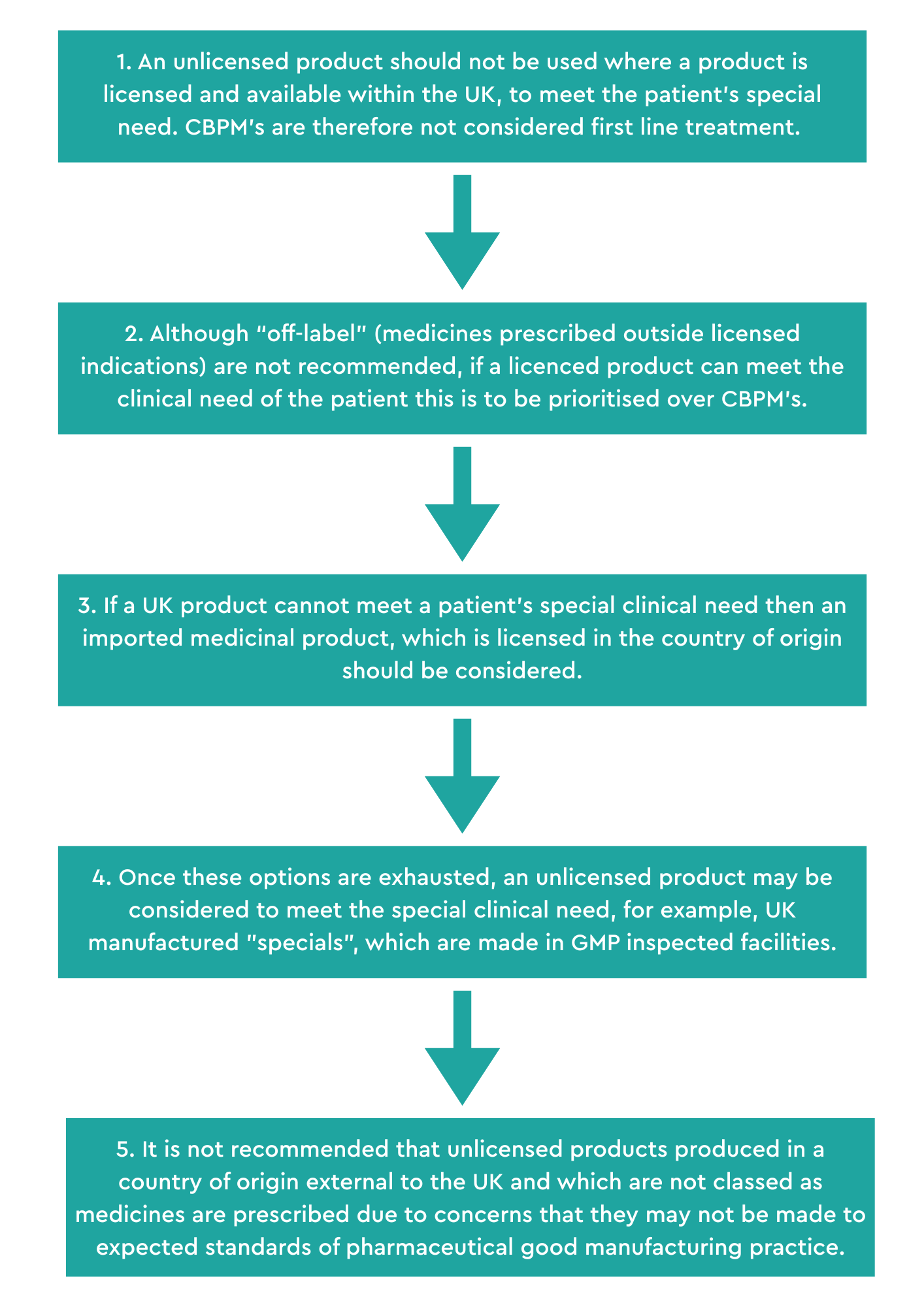
Any decision to prescribe an unlicensed medicine must have regard to the GMC guidance on prescribing unlicensed medicines. The MHRA offer a decision hierarchy for prescribing physicians of unlicensed medicines:
NHS doctors who wish to prescribe unlicensed CBMPs must make an application for exceptional funding, via individual funding requests[7].
Indications for use
For both, licensed and unlicensed CBPM’s, a prescription should only be provided where it is believed to be in the patient’s best interests and when other treatments have not worked or are unsuitable[8].
There is no restriction in law for which indications CBPMs may be prescribed[9]. Prescription of CBPM’s involves a clinician’s judgement having reviewed the patient on a case by case basis.
Contraindications to prescribing
A personal history of psychosis or schizophrenia is the main contraindication to prescribing a THC-containing CBPM[10], THC being one of the psychoactive compounds of cannabis.
Other factors doctors have to consider when prescribing include[11]:
- A history of hypersensitivity to cannabis products
- Cardiac dysrhythmia, especially if may be adversely affected by tachycardia
- Hepatitis C
- Previous or current mental health condition other than psychosis such as mania
- Pregnancy or breastfeeding
- Younger patients less than 21 years – caution required in respect of strength and dosing
- Severe liver disease
- Severe renal disease
- Potential for interaction with other medicines
- History of cannabis dependency syndrome
- History of substance misuse
When prescribing cannabis-based medicinal products for babies, children and young people, clinicians should pay particular attention to the potential impact on psychological, emotional and cognitive development, structural and functional brain development and the impact of sedation[12].
Shared care arrangements
After the initial prescription by the specialist clinician, subsequent prescriptions of CBPM’s may be issued by another prescriber as part of a shared care agreement where it is considered to be appropriate and in the patient’s best interests, their condition is stable and the other prescriber is confident to make an informed prescribing decision about CBPM’s[13].
As part of the shared care agreement it should direct:
- the nature and frequency of monitoring and how this will be recorded
- when treatment might be stopped, for example, if it is not effective
- how suspected or known adverse reactions will be managed
- how communication will be managed between the initiating specialist prescriber, the other prescriber, the patient, family and/or carers
- how the treatment will be funded
- how care will be maintained when the patient, initiating specialist prescriber or other prescriber moves location (including transition to adult services).
The plan should reflect a clear division of responsibilities with specialist initiating treatment still involved in monitoring, evaluation and dose adjustment. It is also expected that decision making will involve a multi-disciplinary team discussion[14].
- NHS OR PRIVATE CLINIC?
Clinicians wishing to prescribe medical cannabis in the UK must be associated with a CQC-registered clinic or hospital[15].
Licensed and unlicensed CBPMs are not routinely prescribed under the NHS. In response to a parliamentary question in December 2024, the government published data on NHS prescriptions for licensed CBPMs. In 2024, 4,326 licensed CBPMs were prescribed[16]. The figures for unlicensed CBPMs were withheld, as these prescriptions were attributed to fewer than 5 patients.
The NHS Business Services Authority has also published data on private prescriptions for CBPMs in response to a freedom of information request. In 2023, it is understood that 182,008 items of licensed CBPMs were prescribed[17]. It is estimated that 45,000 patients are receiving private prescriptions for CBPMs[18].
Currently there is anecdotal data which suggests that access to CBPMs is not keeping up with demand for patients who seek them. For patients, unable to access prescriptions via the NHS, private healthcare costs can outprice those on low incomes or in receipt of benefits[19].
- APPETITE FOR CHANGE?
Under current regulations, only specialist medical practitioners are allowed to prescribe cannabis medicines.
A YouGov Poll conducted in January 2025 found that 73% of the general public believe doctors should be able to prescribe cannabis. Additionally, 83% of MPs also answered that doctors should be allowed to prescribe cannabis for medical use[20]. In Germany, all doctors are able to prescribe medicinal cannabis. Similarly, in Denmark, GPs are able to prescribe[21].
Furthermore, NICE guidelines have been criticised by patients, campaigners and some doctors as limiting, as they do not reflect the current position in the UK[22].
A Westminster Hall debate on the accessibility of medical cannabis took place on 30th January 2025[23]. Shadow Health Minister Dr Luke Evans MP noted, “a recent report by Medcan Family Foundation has highlighted that more restricted prescribing in some areas may be leading to serious or unintended consequences. It is concerning to see, when reviewing their research, that three online forums identified 382 families in the UK who are giving their child illegal cannabis products specifically to manage epilepsy.”
Susan Murray went on to say, “Although, in principle, current regulations permit cannabis prescriptions for severe epilepsy, chemotherapy-induced nausea, muscle stiffness or spasms related to multiple sclerosis, genuine accessibility remains elusive”.
“ By clinging to outdated stigmas, we not only fail our patients but also forgo opportunities to develop a robust medical cannabis sector, stifling both financial potential and essential healthcare advantages.”
The anecdotal and empirical evidence suggests that when people cannot access medicinal cannabis via their doctor, many will go elsewhere, including accessing cannabis via the unregulated market. It is understood that despite medical cannabis having been legalised since 2018, that there are 1.8 million people in the UK accessing the unregulated illicit cannabis market for medical reasons according to YouGov poll commissioned by Sapphire Medical Clinics[24].
Is this enough to improve equality of access
Despite changes to regulations to enable GPs to prescribe being offered as a solution[25], it is felt that there are multiple barriers to access. Many clinicians shared that a major hurdle to prescribing is the lack of good quality randomised control trial (RCT) data demonstrating adequate safety and clinical-cost effectiveness of CBPMs. It is considered by many clinicians that there is a lack of evidence on efficacy, lack of data on long term adverse effects, absence of specialised knowledge and long-term safety data. Many also emphasised an inability to secure funding from NHS trusts[26].
The use of unlicensed CBPMs also place an additional responsibility upon the prescribing clinician, without oversight from regulators, to vet the quality of the product they are providing[27]. Therefore, appetite for further studies and greater licensing of CBPMs is mounting to enable further access.
We will continue to watch this space.















